


GLP-1 agonists for weight loss?
Are semaglutide, liraglutide, tirzepatide or other GLP-1 agonists really the miracle weight-loss drugs?

What is GLP-1?
In order to understand what GLP-1 is, and how GLP-1 agonists work, you first need to know about the basic hormones that regulate energy metabolism in response to food consumption: insulin and glucagon.
WARNING! It’s highly technical, so you might consider skipping next few paragraphs if you primarily digest TikToks.

Insulin
Insulin is a hormone secreted by pancreatic beta cells; it has effects on how your muscle, fat and liver cell work. In general, insulin instructs your tissues to take up glucose while stopping glucose production in your liver. The main purpose of insulin is to “tell” the body that you have reached a fed state. Typically this happens in response to consumption of carbohydrates. In short — you eat carbs, pancreas makes insulin, your liver stops making glucose. Insulin will also regulate the output of the second hormone mentioned above.
Glucagon
Glucagon is a hormone, also produced in pancreas, but this time in alpha cells. It is responsible for instructing your liver to produce glucose. It also increases breakdown of fats and increases ketone production.
As you can see, those two hormones work in relatively balanced relationship (in healthy individuals). When one of the hormones goes up, it regulates the function of the other.
Incretins
Incretins are a group of hormones that are also released in response to food. Their role is to magnify and increase secretion of insulin. Some incretins (like GLP-1) can inhibit release of glucagon. They can also slow absorption of intestinal content into blood stream by reducing the speed at which the food moves from the stomach to the intestines.
In fact, majority (70%) of insulin response after eating food is contributed to the incretins. They are produced in response to glucose and greatly amplify production of insulin. When food passes through the intestines, two main types of incretins are produced in response to glucose contained in the meal.
K-cells in your gut produce GIP (glucose-dependent insulinotropic polypeptide). The L-cells secrete GLP-1 (glucagon-like peptide 1).
How does GLP-1 work?
I have borrowed the images below from this paper (Baggio, 2007).

Both GIP and GLP-1 are responsible for increasing the rate and speed of insulin production in your pancreas. They also increase progenitor cell proliferation in your brain. The key difference is that GIP can increase storage of lipids, and GLP-1 can drive down secretion of glucagon. Another difference (mentioned above already) is that the GLP-1 can slower the rate of stomach emptying, and in result can reduce appetite.
In short — the hormones increase production of insulin and decrease release of glucagon which in turn lowers blood glucose.
High levels of insulin may also “instruct” your tissues to store fat - but more on this later.
GLP-1 agonists
In the late 1980s a group of scientists identified the first GLP-1 agonist (Exendin-4) in animals. Commercially developed GLP-1 agonists (such as liraglutide or semaglutide) are essentially modified Exendin-4. The chemical modification of the molecule is aimed at reducing its rate of degradation (so it acts longer after administration).
GLP-1 agonists were initially developed as medicines for management of type-2 diabetes (as they can have significant impact on stimulating production of insulin by your body).
In the series of 11 clinical trials (SUSTAIN programme) GLP-1 agonists demonstrated improved glycemic control in patients with diabetes (as measured by HbA1c) but also showed a consistent weight loss in trial participants.
More than 10,000 patients with diabetes were given semaglutide and compared to controls, which included placebo, SGLT-2 inhibitors, and other GLP-1 agonists in the case of liraglutide. Semaglutide seemed to perform better in the trials — both in terms of A1C reduction and in terms of weight loss (please note: weight loss, not fat loss!)
In 2021 another semaglutide study gets published in New England Journal of Medicine, where 2000 obese patients (BMI>30) without diabetes were randomised 2:1 to placebo for 16 months. Each participant also received counselling sessions every 4 weeks (with the goal to reduce daily caloric intake by 500 from baseline) and were counselled to exercise for at least 150 minutes per week. The study endpoints looked at the percentage of body weigh change and fraction of body weight lost.

As you can see above, the placebo group participants managed to loose on average 2% of their body weight, while people in the semaglutide group lost significantly more. Around 50% of trial participants lost more than 15%, and a third of subjects lost more than 20% of their baseline body weight. Seems remarkable!
Supplementary findings also showed higher reduction in fasting insulin levels in the semaglutide group (7% vs 26%) and higher reductions in liver function biomarkers (ALT and AST reduction of 11% vs 24% respectively) - however this analysis was performed only in a small subset of patients (n=95 in the intervention and n=45 in placebo group).
The seaglutide group lost 5.25kg of lean muscle mass (1.83kg in placebo), but this is initially not surprising given the larger overall weight loss in the treatment arm. Visceral and total reduction in fat mass was also significantly higher in the GLP-1 agonist treated patients.
Side effects were common in treatment arm, and significantly more pronounced than in placebo groups (44% reported nausea). However, most seemed to be dose-related, and were diminishing over the treatment time. Some can probably also be attributed to the weight loss itself.
What’s the hype?
Obesity is often quoted as a primary cause of numerous adverse health conditions, and is a primary reason for peoples’ dissatisfaction with their external appearance. GLP-1 agonists promise to help achieve and sustain weight-loss with relatively little effort: inject some hormones, your appetite declines, your weight drops. You don’t even need to have diabetes to use them. Magic!
Clever marketing has led to thousands of people starting to use GLP-1 agonists with the hope of looking better on the beach next summer. So many people in fact, that the drug supply in the UK faced severe shortages for months, as the medicine became practically unavailable for people with diabetes. A prescribing guidance had to be developed for GPs to increase chances of sick patients receiving the drug.
There are few GLP-1 agonists available around the world. Semaglutide is sold under two different brand names: Ozempic and Wegovy. It is exactly the same medicine, but marketed to different populations. Both are injectable. Reybelsus (available in some countries) is an oral formulation of semaglutide.
Tirzepatide is slightly different (it is both GIP and GLP-1 - it has lower GLP-1 activity than semaglutide, but much higher GIP activity). It is marketed as Mounjaro, and is not yet approved for management of obesity (only for diabetes). In one study however, it has been shown to be better than semaglutide for weight loss. While a direct comparison is hard (due to differences in study designs), it seems that tirzepatide is a better overall drug for weight loss (and also shows greater reduction in A1C). While injectable semaglutide resulted in average weight loss (at 40 weeks) of almost 7% of body weight, those taking tirzepatide had lost 13% at the same timepoints.
Can you keep your new weight?
If you have read my other posts, you will know that hardly anyone who successfully manages to loose weight is actually able to keep it off, and the vast majority regain everything with a surplus.
Since the GLP-1 analogues have now been studied for some time, there are data emerging showing relatively sustained results over the course 1 year (after 1 year of treatment). At least in patients with diabetes. Data for both agonisers, semaglutide and tirzepatide, start to show trends towards increase in body weight over time (peak reduction around 40-50 weeks since treatment initiation).
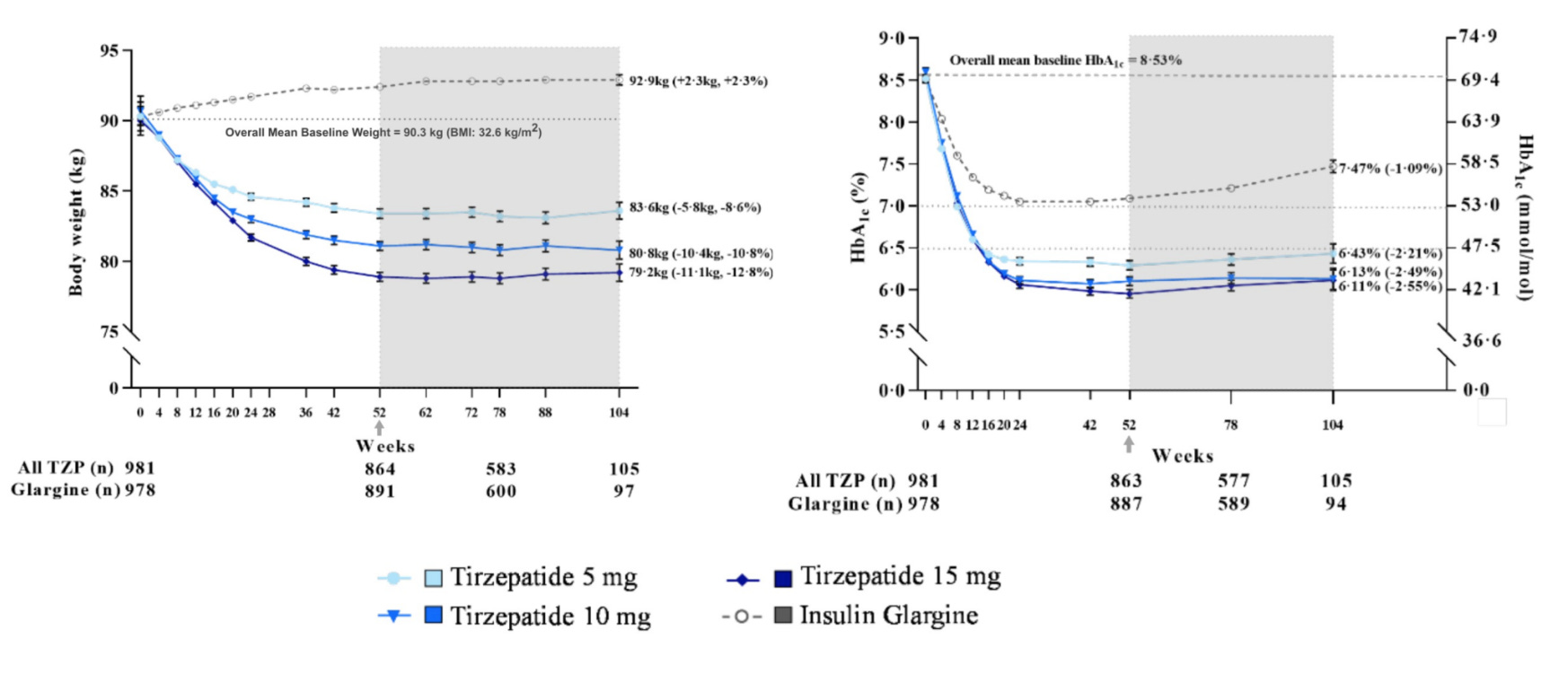
Don’t get me wrong - those trial results are spectacular (at least in patients with diabetes). Note that on the graph above, patients treated with insulin actually put on extra weight when compared to baseline. Results for semaglutide were comparable, but less pronounced. You can also clearly see a dose-dependant effect.
It is impossible just yet to conclude if the weight loss is durable indefinitely - but it is promising. At least in patients with diabetes. And and least in those who stay on the treatment forever…
So what happens when you discontinue the drugs?
If you have read my post “The biggest losers” you already know what to expect. Data is quite clear.

The moment you stop the hormones, you start gaining weight. Rapidly. Irrespective of previous loss. Irrespective of previous dose. It does not reach the starting weight (in the first year) for those who lost more than 20% of body weight, and the gain seems to slow down over time - but it seems that a full weight re-gain is only a matter of time.
There is no data to suggest that the weight regain will not happen. In fact — on the figure above those who have lost 5% of their initial body weight were already heavier after a year than they were at baseline, and those in 5%-10% bracket were back at their baseline weight. Those who lost between 10%-15% of bodyweight were just below their baseline after only 52 weeks from discontinuation of the drugs.
There are plenty of good reasons to believe that for those who lost more it is simply a matter of time before they regain all lost body weight…
Let me tell you why…
…this is really bad for you…
First, let’s talk side effects. Between semaglutide and tirzepatide side effects are broadly similar, but people experience more adverse events and of greater magnitude and duration after semaglutide.
We have already covered the nausea, lightheadedness and reduced exercise thresholds. Other side effects include diarrhoea (up to 30% on semaglutide and 20% on tirzepatide), vomiting (25% vs 12% respectively), constant sinusistis/pharyngitis (up to 20%), headaches (15% vs 6%), abdominal pain (10% vs 5%).
But those are not really problematic. There are some more concerning issues.
Dr Attia and his team reported significant increase in resting heart rate in 100% of people on GLP-1 agonists (approximately an increase of 8-15 beats per minute during night rest). The increase in hear rate also translated into exercise metrics (reported as increase in heart rate during exercise of same intensity and power output as baseline before the start of the treatment). None of those were captured in the clinical trials. They could matter, as your resting heart rate is a proxy for cardiovascular health.
Levels of insulin are elevated in >60% of patients on GLP-1 agonists. Heart rate variability (HRV; a proxy for pending heart failure) also goes down in some patients (it does however go back up when people are taken off treatment).
But by far the most important side effect is related to changes in body composition — namely increase in proportion of fat tissue, and the decline of the total lean muscle mass.
This is profound!
Unfortunately, for some reason, most trials do not track changes in body composition - they focus on overall weight loss only. Only in one of the STEP trials a small subset of patients actually had body composition measured.
Pharmaceutical companies do not track body composition as this is not required by regulators. FDA will only approve a weight loss medicine if the overall weight drops. This is not ideal.
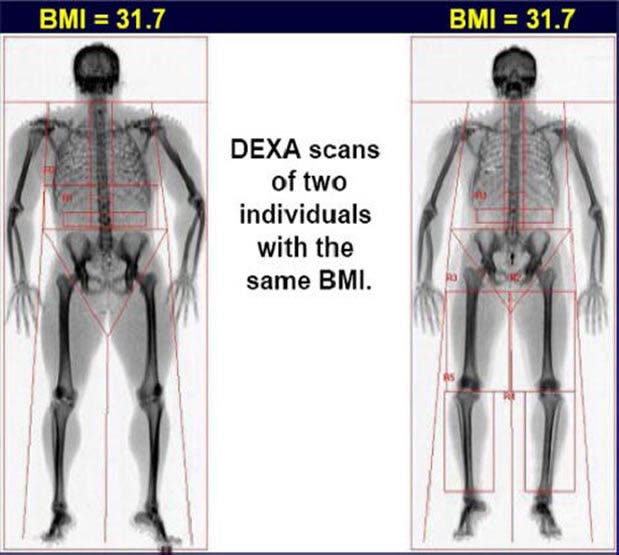
Yes, but why is this bad?
If you clock at 200 kg and loose 20 kg (10% of your body weight) you now weigh 180kg. There is a huuuuuuuge difference between loosing 19 kg of fat and 1kg of lean tissue, and loosing 3 kg of fat and 17kg of muscles. Those weight losses are not the same…
Clinical data indicates that muscle mass loss is very significant in people using GLP-1 inhibitors, despite the requirement to exercise for 150 minutes per week in the clinical trials. And when your weight will eventually go back up — you will regain mostly fat. In the example quoted by Dr Attia, he presents the following case study:
Patient case study (Attia P. et al, 2022)
Female patient with 35% of body fat pre-treatment was initiated on GLP-1 agonists. This represents 80th percentile for her body fat and 75th percentile of muscle mass (adjusted for sex and age).
Following treatment with GLP-1 agonists she has dropped down to 25% of body fat (approximately 50th percentile)
However her ALMI, (Apendicular Lean Mass Index), dropped to below the 10th percentile (anything lower than 50th percentile, is bad!)
This means that the patient went from having quite a bit of muscle mass to being emaciated. Not only the regain in body mass will be significant, she is unlikely to be able to restore her muscle mass, even with lifelong, heavy, daily resistance training, and dramatic increase in protein consumption. And even with such regimen, she might not be able to ever restore the losses.
This would be in stark contrast to how the patient feels after her drug-induced “success”. Would you put your overweight, but overall healthy daughter on such “treatment”? I know that I would not…
Why does it happen? Is this preventable?
Theoretically the loss of lean mass could be prevented, but it is extremely difficult in practice, and therefore impossible (or highly unlikely) for most people.
First of all, every time you loose weight, you will also loose lean mass. With restrictive diet and exercise regimen you can minimise (but not fully prevent) muscle loss. And even if some individuals can do it — it is unbelievably hard.
Furthermore, it is really difficult to stick to a high-protein diet to prevent lean tissue loss, especially if you are also on strong appetite suppressors… Especially since protein-rich foods are the most satiating. Eating a minimum of 2 grams of protein per kg of body weight spread over 4-5 meals a day is much harder than you think when all you feel is nausea.
Now combine this with a likelihood of most people being able to follow a lifelong heavy resistance exercise routine… daily.
So, you will loose weight; and a lot of lean mass; and then you will get all the weight back on - mostly as fat. This will make you sicker. This will make any subsequent attempts to loose fat much harder (read more here).
In other words - if you have enough motivation and discipline to stick to a diet and exercise regimen for life - you likely wouldn’t be obese in the first place… Let it sink in for a moment.
Can things get any worse?
Yes, potentially they can…
Some studies on GLP-1 agonists have suggested increased risk of thyroid cancer (here). The study was done with liraglutide (before semaglutide or tirzepatide were approved). A warning can found in the label as well (GLP-1 agonists may not be used in people with history or family history of medullary thyroid cancer or certain endocrine conditions, like Multiple Endocrine Neoplasias).
Should I use them?
I don’t know. First of all - this is not a place for medical advice. So ask you doctor.
My personal opinion based on available evidence is this: If you want to look good and remain healthy - my gut tells me to stay as far away from GLP-1 agonists as you can.
On the other hand, if you are obese, and have been diagnosed with pre-diabetes, and if you can commit to increased dietary protein intake, and if you can stick to a regular resistance training for the rest our your life - you might be a suitable candidate for treatment with GLP-1 agonists.
Or - in that second case - discuss metformin with your doctor. It has shown similar benefits without many of the risks (here, here or here). Metformin has been used for decades and safety profile is well established. It also costs almost nothing, and has been associated with many additional health benefits and overall reduction in all-cause mortality.