


Psilocybin: 5 Years of psychotherapy in 1 afternoon?
A story about how the US anti-civil right legislation stopped the development of mental health medicines for over four decades.

On a warm summer evening, Albert Hofmann, a chemist employed by the Swiss pharmaceutical company Sandoz (now Novartis), isolated and identified psilocybin and psilocin from Psilocybe mexicana („magic mushrooms”). His team published their results in 1958.
Because Hofmann worked for “the greedy pharma”, his team also successfully synthesised several structural analogues of psilocin to test their effects on humans. And the effects were nothing short of astonishing.
Hofmann’s research led to the discovery and development of synthetic psilocybin (quick to make, easy to store, precise to dose), ethocybin and a compound CZ-74. Not only did their physiological effects last half as long as psilocybin, but the pills were easy to correctly dose and praised (especially ethocybin) for lack of any signifiant adverse reactions.
Soon after the pharmaceutical discovery, Harvard University became the world’s largest testing ground for psychedelics, including psilocybin. Dr Timothy Leary obtained synthesised psilocybin from Hofmann via Sandoz Pharmaceuticals. Early research of Metzner and Leary (including the Concord Prison Experiment) suggested positive results of the substance in clinical psychiatry.
Unfortunately, the potential for psychedelics to reduce an individual’s ego, increase altruism, and invoke the feelings of love and acceptance towards all living creatures was not exactly in line with the struggle of Uncle Sam to increase the number of cannon fodder recruits in the US Army… Especially, as the US war machine needed many recruits for the wars in Vietnam, Cuba, Guatemala, Colombia, or to manage the ongoing threat from the Soviet Union.

In 1966, the United States drove a nail into the coffin of scientific research on psychedelics. The US government passed laws that prohibited the production, trade or ingestion of hallucinogenic drugs. Sandoz, threatened by sanctions, stopped production of psilocybin and LSD the very same year…
Further restrictions were imposed by Congress in 1970, which made it illegal to use psilocybin for any and all purposes (including scientific research). This has stopped the research of potentially promising treatments for multiple mental health conditions for over 50 years…
What were they so afraid of?
What even is psilocybin?
Psilocybin is a biologically inactive compound produced by various species of fungi, commonly known among enthusiasts as magic mushrooms. Following ingestion of psiolocybin-containing substances, such as any of the 200 different kinds of magic mushrooms, psilocybin is converted in our bodies into psilocin, which has hallucinogenic effects similar to other hallucinogenic compounds: tryptamines, phenethylamines or lysergamides (think: DMT, MDMA, mescaline, LSD, etc).
Psilocin administered orally to humans induces euphoria, visual hallucinations, mental hallucinations, changes in sensory perception (visual, auditory, proprioceptive), disorientation, distorted sense of time (or lack of ability to track time), perception of spiritual experiences, joy or depression, nausea, paranoia (usually transient), panic attacks. It has been shown to intensify affective responses and enhance users’ ability for introspection. It also causes regression to childlike thinking and activation of vivid memory traces. Visual hallucinations (closed-eye and open-eye) are common, but relatively rarely confused with reality.
The scope and duration of those effects depend on the species of mushrooms, ingested dose, individual physiology and genetics, but also on non-pharmacological parameters, such as the location of the patient, set and setting (including company, mood, ambient temperature, lightning, etc), loudness of the environment, presence of other people, and so on.
Is it toxic?
Not as much as cyclists.
Typical responses to psilocybin include tachycardia, dilated pupils, arrhythmias, hypertension, general instability, tremors, and vomiting. Repeated, daily dose escalation (for up to 21 days) does not appear to have any measurable impact on blood glucose, or electrolyte levels, and does not alter liver toxicity tests (despite being metabolised in the liver).
More robust toxicity data is limited, however last decade brought a steady increase in recorded cases of psilocybin overdose. Overall, the hospitalisations remain very rare, and most overdoses are self-limiting. Acute management protocols focus on the management of immediate adverse events (such as anxiety or paranoia), rather than any pharmacological interventions.
Lethal dose in rats (LD50) following oral administration of psilocybin is approximately 280mg/kg of body weight. To put that into context: it is 50% higher than for caffeine. Since psilocybin comprises ca. 1% of the weight of an average “magic” mushroom, an average person (if they were a rat) would need to eat in excess of 1.5kg of dried (or 15kg of fresh) mushroom to die.
Because humans are not rats (well, at least biologically) the lethal dose is actually extrapolated to approximately 6 grams. Since an “effective” dose is as low as 6mg (0.006 grams), the therapeutic window is relatively large (3 times larger than for aspirin, or 30 times as wide as for nicotine).
There were 2 reported deaths in literature (as of 2011) attributed to an overdose of “magic” mushrooms. Tolerance builds quickly and dissipates just as fast (within 7-10 days), and repeated use does not appear lead to physical dependence.
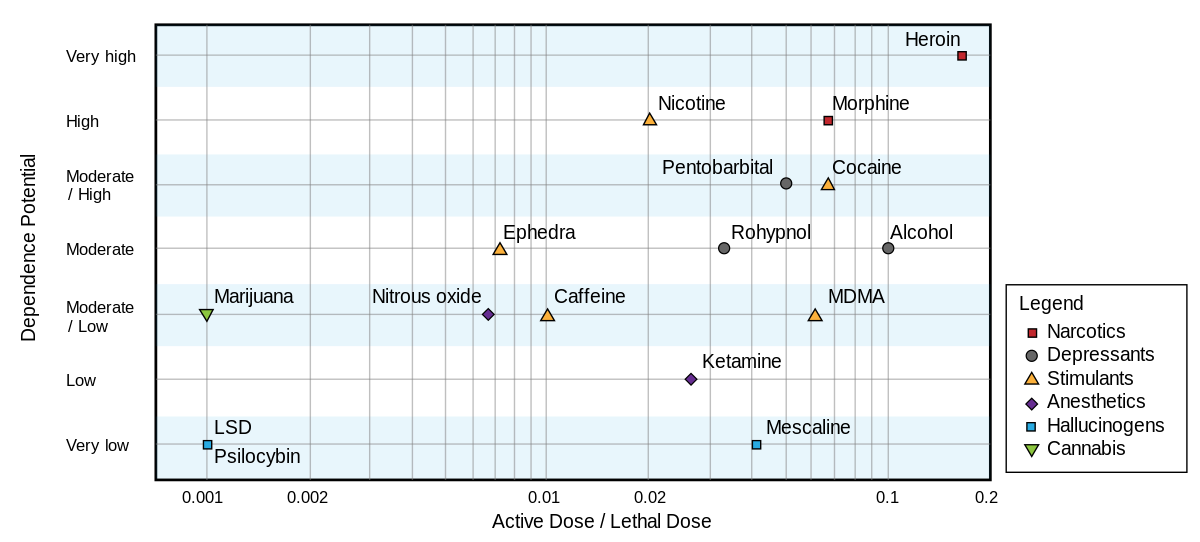
Some researchers in the UK ranked psilocybin as the illicit drug with the lowest harm when compared to other recreationally consumed substances. This was also confirmed by Dutch scientists. But because researchers in Britain had better friends, their results got published in the Lancet, while the Dutch had to print in something called Eur Addict Res, which nobody ever heard of.
How does it work?
By mimicking the “flooding” of your brain with serotonin.
Technically, psilocin acts as a 5-hydroxytryptamine (5-HT) receptor agonist. Because there are few types of 5-HT receptors, the psychosis-like effects of psilocin can be blocked by ketanserin (5-HT2A receptor antagonist). Research shows that interaction with non-5-HT2 receptors may still provide “benefits” (subjective and behavioural) without hallucinations.
Unlike LSD, psilocybin (psilocin) does not bind to dopamine receptors, but can indirectly increase the concentration of dopamine in certain parts of the brain.
The effects start after approximately 30 minutes (+/- 10 minutes) from oral ingestion, and last approximately 4 hours (+/- 2 hours) depending on the dose and individual genetics. The half-life is approximately 2.5 hours (+/- 1 hour).
The main problem with “amateur dosing” is related to the unpredictability of psilocybin content per mushroom, which can vary from 0% to 2.5% of dry weight and depends on species, strain, growth condition, maturity at harvest, drying conditions, mushroom size, and can vary even in between individual mushrooms grown from the same strain.
It is legal?
No.
Possession of psilocybin-containing substances is illegal in most countries, as psilocybin is classified as a Schedule I controlled substance under the 1971 United Nations Convention on Psychotropic Substances.
Despite being illegal in many Western countries, such as the UK, Australia and some US states, less conservative governments opt to nurture the legal use of psilocybin and other psychedelic drugs. In the Netherlands, authorities provide education and promotion on the safe use of psychedelic drugs, such as psilocybin, to reduce public harm. From 1 July 2023, the Australian medicines regulator has permitted psychiatrists to prescribe psilocybin for the therapeutic treatment of post-traumatic stress disorder (PTSD).
Why is it illegal?
History teaches us that quite often a decision to restrict the use of (or limit the research of) any substance is politically driven and aims to restrict, punish or persecute certain groups of people.
For example: the first anti-opium laws in the 1880s were aimed against the Chinese labourers who came to build the railroads in the US. Marijuana prohibition was mostly aimed against Mexican and African American users of cannabis in the USA. The psychedelic crackdown in the 1960s was against the hippies (who were largely opposing the US war machine at that time).
John Ehrlichman, a military serviceman, who was Nixon's domestic policy advisor, famously said that the White House had two major enemies, and one of them was the Civil Rights Movement (more here, and here)
“The Nixon campaign in 1968, and the Nixon White House after that, had two enemies: the antiwar left and black people. You understand what I’m saying? We knew we couldn’t make it illegal to be either against the war or black, but by getting the public to associate the hippies with marijuana and blacks with heroin, and then criminalizing both heavily, we could disrupt those communities. We could arrest their leaders, raid their homes, break up their meetings, and vilify them night after night on the evening news. Did we know we were lying about the drugs? Of course we did.”
- J. D. Ehrlichman
Nixon’s anti-drug policy criminalised any use, production and research of all psychedelics, and also “successfully” wiped out significant and promising mental health research, both in the United States and around the world. For decades.
In 1985 the DEA (Drug Enforcement Agency) criminalised the use of MDMA, despite being in the middle of being sued to keep MDMA legal as a medicine. Believe it or not, the DEA lost the court case but proceeded to delegalise, arrest and prosecute users, as well as doctors and researchers.
Surprisingly, many other controlled substances (like amphetamines, cocaine or opiates) were still allowed to be made and used and were never the target of any DEA raids. Why? Most likely, because of their abundant and significant utility in… combat medicine and wide use among deployed military personnel.
In 1992, the FDA had a special advisory committee meeting and they decided to reopen the door to psychedelic research. This move was forced by the AIDS community. The massive protest outside of the FDA headquarters was successful, the whole building was shut down, which later forced the administration of the FDA to create what was called the “Pilot Drug Evaluation” program. The program no longer exists, but it laid the foundations for researching scheduled drugs.
Today, we have approximately 5 times more new clinical trials for psychedelics than they were in the 1960s. Let’s hope they will bering long awaited improvements in mental health care.
What are potential research directions?
Before the research became illegal in the 1960s, and from limited research conducted after the year 2000, multiple potential clinical applications were proposed. Psilocybin has been investigated for its possible role in the treatment of:
Personality disorders,
PTSD (Post-Traumatic Stress Disorder),
Nicotine addiction (tobacco smoking),
Alcohol dependence,
OCD (Obsessive-Compulsive Disorder),
Cluster headaches and migraines,
Cancer-related distress and end-of-life care,
Anxiety disorders,
Mood disorders,
Treatment-resistant depression (TRD),
and others.
Why do people take it?
Hallucinations aside, a prospective study from 2011 suggested that psilocybin can cause long-term changes in the personality of its users, namely by increasing the “openness” dimension of the revised NEO Personality Inventory. Studies further report that many subjects experienced long-lasting (more than 12 months) changes to traits like altruism, gratitude, forgiveness, and feeling close to others when psilocybin was combined with regular meditation practice.
A 2009 national survey of drug use by the US Department of Health and Human Services concluded that the number of first-time magic mushroom users in the United States was roughly equivalent to the number of first-time users of cannabis. In European countries, the lifetime prevalence estimates of psychedelic mushroom usage among young adults (15–34 years) range from 0.3% to 14.1%.
What is “Ego Dissolution”
Loss of subjective self-identity.
This is one of the possible effects of ingesting psilocybin and is typically temporary. Alnaes (1964) defines ego death as "loss of ego-feeling", while more modern researchers describe it as “temporarily experiencing a complete loss of subjective self-identity”.
The importance of this is unknown, but could be partially responsible for the reported “benefits” of using psilocybin.
What are Psychoplastogens?
A group of SMDs (small-molecule drugs) that produce rapid and sustained effects on neuronal function and/or neuronal structure manifesting as a therapeutic benefit after administration of a single dose.
Psilocin is one of the identified psychoplastogens, alongside ketamine, MDMA, scopolamine, LSD or DMT, ibogaine, tabernanthalog, AAZ-A-154, rapastinel, and a few others. Those compounds have the potential to rapidly promote neuronal changes as recently demonstrated in clinical research.
At the moment, the only FDA-approved psychoplastogen is esketamine (sold by Janssen Pharmaceuticals) and licensed for management of treatment-resistant depression and suicidal ideation.
Neurotoxicity or neuroplasticity?
For many decades psychedelics were described as neurotoxic - assuming that any change in the brain is inherently bad. Psychedelics, including psilocin, have been suggested as substances that can restore neuroplasticity of the brain - introduced changes to neural pathways that are largely beneficial to the patient.
Gould Dolan at Johns Hopkins has shown that the length of time that you're in the psychedelic experience extends long afterwards the session is complete. To explain this phenomenon she coined the phrase “critical periods” for the brain.
For example: children can learn languages easier than adults because they are in a “critical period” of language development. Dolan believes that there are other critical periods for learning different things throughout life. Later, in adulthood, most people function on already developed patterns of behaviour. Dolan suggested that by “resetting” certain pathways in the brain with psychedelics, adults can easily re-learn new behaviours and create new response pathways in their brains.
Because the effect of psychedelics can last for weeks after the administration of the treatment, the therapy should have a dual focus: the “initial experience” and the “integration work” typically achieved via therapy (assisted or self-guided), meditation, reflection and re-learning of new behaviours and patterns to build new neural connections.
A good example of the “dual focus” in treatment is illustrated by the use of psychedelics in the treatment of PTSD: psychedelic-assisted therapy. Psychedelics can be used as a tool to rapidly rewire the brain. There is a risk that the user might end up in a worse place than at the start if the environment is not supportive or conducive to inducing a lasting positive change. It's not like you take MDMA and everything's fine.
Things are a bit more complex…
MDMA reduces activity in the amygdala, the fear-processing part of the brain - which makes MDMA the psychedelic of choice for PTSD (fear-induced trauma). MDMA also increases activity in the prefrontal cortex - the part of the brain that some of us use to think logically. One of the “features” of PTSD is that episodes are triggered by your reminders of traumatic events - a pathway that can trigger certain reactions in response to a loud sound (which is maladaptive when soldiers return to civilian life). The neutral pathway created during extreme, life-threatening events, changed the patient’s brain: they now have a hyperactive amygdala where the fear is processed, combined with the reduction of activity in the prefrontal cortex (so sufferers are not logically thinking and evaluating each loud sound). This results in permanent changes to the hippocampus, where we put memories into a “long-term storage”.
As MDMA reduces activity in the amygdala, increases activity of the prefrontal cortex and facilitates forging new paths in the hippocampus, allowing new pathways to form and new, more adaptive behaviours to emerge, provided that the environment is supportive of such a change.
Think of replacing years of psychotherapy with a single, psychedelics-assisted session…
Shouldn’t we all be taking it?
No.
First of all, there are side effects. Some were mentioned already above. Panic, paranoia or psychosis seem to be a bit more concerning. Long-term negative outcomes are also poorly described, and typically come from self-reported studies. “Bad trips” and other “harmful” experiences appear to be more common in women.
Microdosing (taking very small doses, but regularly) seems to carry a significantly lower risk of adverse outcomes. It also seems to alleviate cluster headaches, and allows to avoid all psychoactive effects of the drug.
What else?
I very much care about objective reality. Science did not achieve maturity until we were able to successfully either extend the reach of our senses (with microscopes, telescopes, machines that read), or replace our senses (invent things that sense the world in ways we don't even have senses to notice).
The available evidence hints that psychedelics may be helpful for someone who is in need of some “repair” in their brain (like PTSD, depression, anxiety, trauma, etc). They might also have an appeal to spiritual people, as it may make them feel even “more spiritual” in whatever way that manifests.
There is absolutely no evidence that psychedelics can expand our senses or extend our understanding of the objective reality. While the dissolution of certain cortical pathways may help to enhance a creativity of an artist, it is unlikely to push our understanding of objective reality (and therefore since) any further. I'm not denying that this could trigger creativity in the artist…
Can people have completely new ideas under a non-ordinary state of consciousness? Can magic mushrooms advance humans to better understand our objective reality?
There are no evidence-based answers to those questions. Some researchers believe that at least certain ideas, even in physics, mathematics and other “hard” sciences are insights. And if non-ordinary states of consciouness could produce insights that could take our thinking outside of our previous boxes, perhaps there is something to look for?
A Stanford University’s pilot study conducted in the mid-1960s used mescaline and LSD in people that had unresolved, objective problems with their business or science problems. Volunteers were given the above mentioned psychedelics in order to help them try to resolve some of these problems. Tentative findings suggested that, if given according to a carefully structured regimen, psychedelic agents seemed to facilitate creative problem-solving. The pilot study was never completed due to the legal bans. However, Jim Fadiman, who planned this research, is today one of the main advocates of microdosing of psychedelics among academics and scientists….
If you’d like me to add more details on micro-dosing, “fun dosing”, and dosing for assisted-therapy, just leave a comment!